The following is from the latest issue of the Full Stop Quarterly. You can purchase the issue here or subscribe at our Patreon page.

Sometime in 1851 a group of Americans arrived at Cruces, Panama, New Granada returning east from the goldfields of California. The rowdy travelers crowded into the Independent Hotel, a dining and lodging establishment operated by a Jamaican entrepreneur who had arrived in Panama a year or two previously. There they dined on slapjack, “a thick substantial pancake of flour, salt and water . . . followed by pork, strips of beef stewed with hard dumplings, hams, great dishes of rice, jugs of molasses and treacle for sauce, the whole being washed down by an abundance of tea and coffee.” With dinner concluded, the evening gave way to singing, dancing, and revelry, as the locals did their best to separate the American travelers from as much of their newfound gold as they could in one evening: “these few hours of gaiety and excitement were to provide the Cruces people with food and clothing for as many days.” The local economy was booming, for Panama had become a crossroads of interoceanic travel and the fastest route to Gold Rush California.
Long before the Panama Canal was built (but long after the project of a canal had first been imagined), the discovery of gold in California transformed the Panamanian transit zone. This narrow strip of land stretching along the river Chagres from Colón, on the Atlantic Coast, to Panama City, on the Pacific, had for centuries been a principal site of interoceanic crossing, used by the Spanish Empire to transport South American gold to waiting galleons for the return trip across the Atlantic to Spain, and then by Panamanian merchants facilitating the movement of European trade goods from the Caribbean to the Pacific. But the Gold Rush brought travelers through Panama as never before as Americans eager to try their luck in California discovered that the path across the isthmus represented the shortest route. Soon, American capitalists began building a railroad across Panama, one that would shorten the travel time between the coasts from several days to several hours. Yet while the railroad was under construction, the transit zone continued to prosper, spawning a host of businesses operated by locals and emigrants offering transportation, lodging, food, provisioning, and entertainment to gold seekers, traders, and railroad construction employees alike.
The scene above played out in Cruces four times a month as new groups of travelers passed through town on the way to or from Panama City. Yet this occasion was not entirely a typical one, because, shortly after the American travelers departed, the residents of Cruces “found that they had left one of their number behind them: the cholera” (29). Cholera, the pandemic disease of the nineteenth century, was circling the globe for the third time when it arrived in Panama in 1849, probably transported by a steamship from New Orleans. Across the world, nineteenth-century life was punctuated by no fewer than five cholera pandemics, each lasting years before abating only to give way to a fresh wave of infections. From Asia to the Americas people tracked the progress of the disease from region to region and town to town, hoping and, in many cases, literally praying that their area would be spared. By the end of the century, very few places on Earth had been. Millions died.
We know the details of the outbreak in Cruces thanks to the writings of Mary Seacole, a Jamaican Creole healer whose memoir, The Wonderful Adventures of Mrs. Seacole in Many Lands, stands as a classic of Victorian travel, war, and medical literature. Seacole became famous in 1850s Britain for her time as a sutler—a private merchant specializing in the provisioning of soldiers on campaign—at the siege of Sebastopol during the Crimean War. Yet she has recently become revered as an early hero of the nursing profession thanks to her ministrations to sick and dying British soldiers on the battlefield. Though her actions at Sebastopol and the favorable coverage they received by the British periodical press made her famous, Seacole developed her skills as a nurse and as a caregiver in the Caribbean and Central America during the cholera’s deadly emergence in Jamaica, in 1850 and 1851, and later in Cruces in 1851 and 1852. After the outbreak of cholera left Seacole’s hometown of Kingston devastated, she traveled to Panama to follow her brother into business as the proprietor of a dining and hospitality establishment catering to gold rush travelers.
During the years from 1848 to the outbreak of the American Civil War, many, like Seacole and her brother, traveled from across the world to seek fortunes—not only in the California goldfields, but in the boomtowns of the isthmus. These new arrivals mingled with locals, who had profited from their geographical position along a major international trade route since the sixteenth century. While some, like the Seacoles, became independent proprietors, many others, especially manual laborers from China and Jamaica, went to work building the Panama Railroad, which opened in 1855, at the cost of thousands of workers’ lives. Panama was a space of economic opportunity and, as portrayed by European and US journalists, of exhilarating technological progress. Yet it was also a place where people were dying en masse, not only from cholera but also from yellow fever, malaria, and suicide. The circumstances surrounding the Panamanian cholera, Mary Seacole’s presence in Panama, as well as the account she authored of her role in treating its victims, present a portrait of one epidemic-stricken community that responds in ways both typical and, in our own pandemic times, uncomfortably familiar. The circumstances of cholera’s arrival in Panama—and of Seacole’s presence there—similarly recall the ways that all pandemic diseases rely on human activities to propagate: They move with their hosts, along trade routes and waterways, through military camps and religious gatherings. Panama became what it was during the gold rush years thanks to a unique confluence of nature and commerce. Eventually its residents would suffer the predations of a disease spread by global capitalism in a pandemic directly produced by the same British military adventurism Seacole would later devote her mature life to serving.
Cholera first appeared in India; the microbe that causes the disease is endemic to the Ganges River Delta. Though the disease had been attested for centuries, it had never before spread beyond its local area. In a nineteenth-century world crisscrossed by commercial and imperial expansion, however, these localized epidemics soon turned globally pandemic. Beginning in 1817, the first cholera pandemic spread to many parts of Asia, aided by the movements of British armies and local religious pilgrims, reaching both China and the Eastern Mediterranean before abating in 1824. By 1828, cholera had returned, sweeping through India, China, Japan, and the Middle East before reaching Russia and then moving from Russia to Europe and then to North America, petering out in 1834 after having nearly circumnavigated the globe. Latin America had been spared, but that was to change less than two decades later when a third, even deadlier, pandemic again emerged in 1846. Twenty-nine years after 1817, the world was even more closely knit together by global trade and globalizing empire; this time, the disease spread faster and farther than before, touching every continent but Antarctica and not abating until 1863. The third pandemic was the first to hit Latin America and most of the Caribbean, though Cuba had sustained an earlier brush with the disease in 1834. Spread by extensive maritime trade as well as military activity, the third cholera pandemic eventually touched “Jamaica, Cuba, Puerto Rico, St. Thomas, St. Lucia, St. Kitts, Nevis, Trinidad, the Bahamas, St. Vincent, Granada, Anguilla, St. John. Tortola, the Turks and Caicos, the Grenadines [. . .] and possibly Antigua.” Conservative estimates put the global death toll of the third pandemic alone in the hundreds of thousands.
Because Panama was already a hotspot of global travel, cholera hit the isthmus particularly hard. Panama had long endured a reputation for infectious diseases, which would continue until the twentieth century, when the United States Canal Authority pioneered a set of innovative actions against mosquitoes that drastically reduced yellow fever infections and nearly eliminated them within the Canal Zone (cholera would fall victim to this same sanitary program, finally disappearing from Panama in 1906). But cholera, unlike yellow fever, is not spread by mosquitoes, nor is it in particular a tropical disease: It originates in drinking water contaminated by the feces of infected people, and throughout the early and mid-nineteenth century, before germ theory, the disease was practically impossible to combat effectively. To make matters worse, the few scientists who seemed to have an idea of how to control it were either marginalized or ignored.
In Cruces, there is no ignoring the timeline of the disease’s emergence, which claims its first victim not long after the American travelers’ departure. Seacole narrates the first patient’s death: “A Spaniard [a Panamanian], an old and intimate friend of my brother, had supped with him one evening, and upon returning home had been taken ill, and after a short period of intense suffering had died. So sudden and so mysterious a death gave rise to the rumor that he had been poisoned, and suspicion rested for a time, perhaps not unnaturally, upon my brother. [. . .] I went down to see the corpse. A single glance at the poor fellow told me the terrible truth” (30). Accounts of cholera infection across the nineteenth-century world often begin this way: A single victim is discovered to have a mysterious illness, which progresses rapidly and soon kills. As one study of cholera in Jamaica observes, “histories of great nineteenth-century cholera epidemics often resemble good horror stories,” and the first cases produce widespread panic, leading to people fleeing cities and towns, further spreading the disease: “soon whole cities were silent save for the rumble of the ‘dead-carts’.” By the 1850s, the average person living in the Caribbean had a very high chance of having lived through an outbreak in their community or in one nearby, and would certainly have heard or read about infections across the region. Cholera outbreaks made for dependable news coverage because the disease’s spread was so unpredictable, its emergence so sudden, and the deaths it caused so swift and terrible. Confronting the epidemic in Cruces, Seacole describes the incredible suffering that the victims of cholera experienced, usually very quickly after the onset of symptoms:
Generally speaking, the cholera showed premonitory symptoms; such as giddiness, sickness, diarrhea, or sunken eyes and distressed look; but sometimes the substance followed its forecoming shadow so quickly, and the crisis was so rapid, that there was no time to apply any remedies. An American carpenter complained of giddiness and sickness—warning signs—succeeded so quickly by the worst symptoms of cholera, that in less than an hour his face became of an indigo tint, his limbs were doubled up horribly, and he died (35).
To make matters worse, the etiology of the disease as well as the mechanisms by which it spread remained contested until the 1870s. Though medical professionals argued as early as the first pandemic that the disease was contagious, without a germ theory of disease the link remained a subject of significant debate. Without any way of identifying the cause of the illness, nor understanding how to effectively prevent people from contracting it, the treatment remained essentially supportive and symptomatic. Seacole, for example, describes a program of painkillers and purgatives designed essentially to minimize suffering while expelling harmful elements from the body. Some of these practices were woefully misguided; in some cases, patients who received treatment were more likely to die than those who received none at all, since they tended to accelerate the dehydration that caused death in choleric patients.
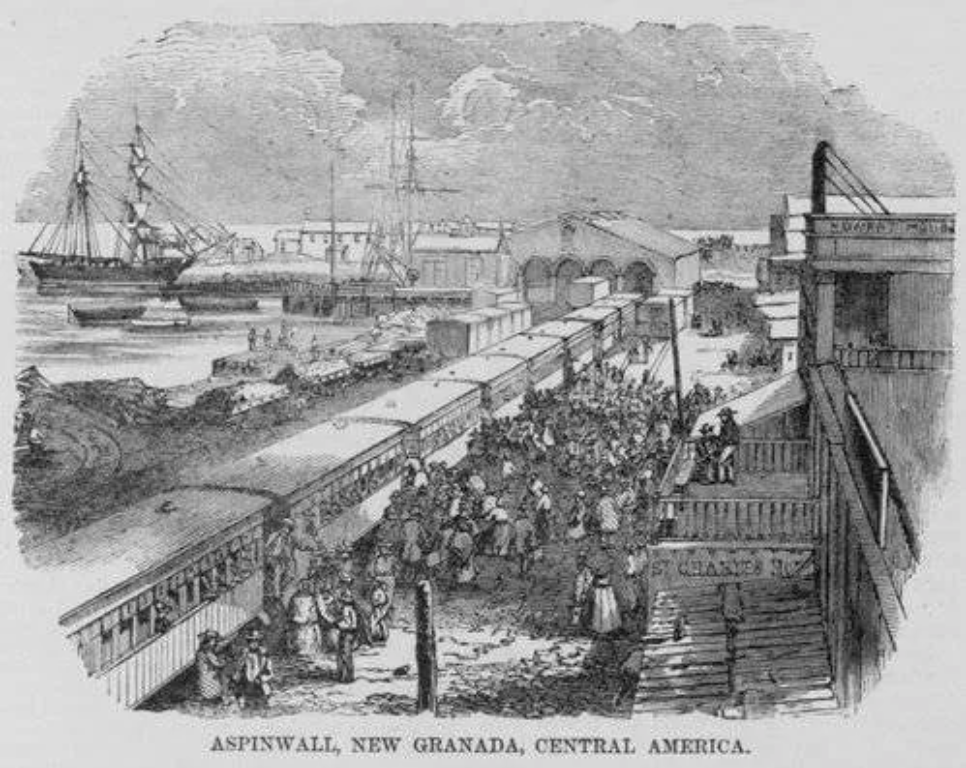
Mary Seacole’s treatments—“mustard plasters, and emetics, and calomel; the mercury applied externally . . . water with cinnamon . . . warm oil, camphor, and spirits of wine” (34–45)—are more palliative than curative. However, they represented the best that local and traditional medical knowledge could mobilize to combat the sickness. These techniques emerged as the hard-won results of first-person experimentation, as practitioners tried desperately to save patients and or at least provide some measure of comfort. Though the British physician John Snow famously discovered that cholera spread through contaminated drinking water by pioneering epidemiological mapping in London just 2 years earlier, in 1849, his discoveries were rejected by many in the traditional medical establishment. In Cruces, a frontier town far from the hospitals in Panama City and Aspinwall, the situation was worse still: An incompetent dentist was the sole representative of the medical profession, and “the people soon saw that he was not familiar with the terrible disease he was called upon to do battle with, and preferred trusting to one who was” (31). Seacole had lived through the Jamaican cholera epidemic of 1850–1851, which arrived from Jamaica on a steamer from Panama, likely traveling with Jamaican workers returning home from working on the Panama railroad, another illustration of the ways that people in the Caribbean were knit together by the ties of trade and travel, and now by the experience of disease. In many cases lay survivors had a better account of how and why cholera spread than physicians still beholden to a sanitary model that blamed miasmas—bad air—and noxious vapors for propagating the disease. As Seacole writes, Jamaicans knew better: “I believe that the faculty have not yet come to the conclusion that the cholera is contagious, and I am not presumptuous enough to forestall them; but my people have always considered it to be so” (29). Thus Seacole brought with her to Panama a lived expertise in the treatment of cholera as well as the perspective of a person who has already survived one devastating epidemic. Seacole thus draws our attention to an emerging community of survivors who could be counted on to guide cholera-naive populations through their own outbreaks.
If Seacole threw herself into combating the outbreak, it does not mean that she later evaded expressing typically British cultural prejudices back to her British readership (especially since—as Pamela K. Gilbert has documented, in Cholera and Nation: Doctoring the Social Body in Victorian England—from the very first cases of cholera in Britain, the disease was associated with non-Anglican populations, like the Irish Catholic working class and the Scottish Presbyterians, and even blamed on Britain’s growing religious tolerance). Thus Seacole, even as she laments the fate of the Panamanians struck down by cholera chastises their superstitious response: “Beyond filling the poor church, and making the priests bring out into the streets figures of tawdry dirty saints, supposed to possess some miraculous influence which they never exerted, before which they prostrate themselves, invoking their aid with passionate prayers and cries, they [the Panamanians] did nothing” (31). The Spanish doctor has failed his charges, and the Catholic church has done so as well (never mind that the British themselves responded to the earliest cholera pandemics with national days of fasting and prayer!). Even in the best of times, New Granada’s grip on political sovereignty and the institutions of government in Panama were fragile, and doubly so in the transit zones. So every institution of social life has failed or abandoned the people of Cruces in their time of greatest need, leaving them to confront the pestilence with only the aid of “the yellow woman from Jamaica with the cholera medicine” (31).
By presenting herself as the only one capable of combating the cholera when everyone else had failed, Mary Seacole rejects common understandings of cholera as a disease both racialized and gendered. As Gilbert explains, by 1866 Britons feared the cholera as “an alien enemy from the colonial lands that attempts to ‘penetrate’ and lodge itself in British soil” (120). This was the view that had begun to emerge by the late 1850s, when Seacole’s memoir was published. Cholera was reframed as an alien, racialized other from the peripheries of the Empire around the same time the Indian Mutiny of 1857, a major rebellion against colonial rule, began to harden British racist attitudes towards colonized people, chief among them the Indians (Upon returning from Crimea, Seacole put together a company of forty nurses to travel to India and nurse soldiers engaged in suppressing the Indian Mutiny of 1857–1858. In all probability she was never able to follow through with this plan.) The Morant Bay Rebellion, which occurred in Jamaica just eight years later, would similarly inflame anti-Black racism among the British public. Britons were beginning to understand that, though cholera could become epidemic in many places, it had its origins in India. They remained much less convinced of the British Empire’s, and particularly the British Army’s, own role in facilitating its spread. Moreover, though nineteenth-century understandings of how and why cholera appeared and spread differed across ideology and changed over time alongside medical opinion, bourgeois attitudes tended to fixate on the personal behavior of cholera victims as implicated in a person’s susceptibility to the illness. This was true of the Manchester slums, where repeated cholera epidemics ravaged working class residents across decades. It was equally true in the Caribbean, where Black people suffered much higher mortality rates than whites across every outbreak thanks to poverty, insufficient sanitation in Black neighborhoods, and comparatively poor nutrition. (The stark racial inequalities associated with death from pandemic disease are as true today as they were then, as reflected in the ongoing COVID-19 pandemic). Seacole pushes back against the racialized and gendered associations of causation and susceptibility to cholera by emphasizing the Creole healing tradition in which she was educated, her extensive personal experience treating cholera, and her long service to the British Army. Yet her account of the personal behaviors of Panamanians serves to perpetuate many of these same associations, even under the guise of social critique. Taken together, these excerpts from Seacole’s account highlight her status as both a dedicated caregiver, and, at the same time, a devoted partisan of the British Empire, one who, as Sarah Salih writes in her article “‘A gallant heart to the empire.’: Autoethnography and Imperial Identity in Mary Seacole’s Wonderful Adventures,” endorses “an affective imperialism in which she plays [. . .] a nurturing and supportive role” (175).
The cholera’s arrival has the effect not only of upending the normal social order and the rules of life, but also of highlighting them in all their absurd arbitrariness. In this respect, Seacole’s account of the suffering and death of a wealthy “New Granada grandee” and his wife is illuminating:
It was when the cholera was at its height, and yet he had left—perhaps on important business—his wife and family, and gone to Panama for three days. On the day after his departure, the plague broke out in his house, and my services were required promptly. I found the miserable household in terrible alarm, and yet confining their exertions to praying to a coarse black priest in a black surplice, who, kneeling beside the couch of the Spanish lady, was praying, (in his turn) to some favourite saint in Cruces. The sufferer was a beautiful woman, suffering from a violent attack of cholera, with no one to help her, or even to take from her arms the poor little child they had allowed her to retain. In her intervals of comparative freedom from pain, her cries to the Madonna and her husband were heart-rending to hear (36).

Seacole points to the Catholicism of the residents as an impediment to scientific treatment of the disease; even on the point of death, the members of the household are more responsive to the priest than to Seacole. This behavior presents an explicit contrast with Seacole’s own pragmatic approach to treatment: Mere pages earlier, she bribes a local to assist her in performing an ad-hoc autopsy on the body of a recently deceased child she had been nursing, in order to better understand the progress of the disease (34). Yet for all Seacole’s ministrations, she is powerless to save the wife of the grandee. When city authorities come to collect the body and cart it off to be buried, household “relatives and servants” (36) bar the door and refuse to allow the burial gang to enter until the corpse of the deceased woman can be dressed up in a white satin gown, because the household’s pride of station prohibits the wife’s being buried without the trappings of her social rank, even as Seacole struggles to save the infant, who soon makes the journey “to join its dead parent” (36). The scene presents in microcosm all the terrible chaos and wrongheadedness of the town’s response to cholera: The head of the household has fled, his wife lies dead, Seacole, forgotten, struggles in one corner of the room to save their dying baby, the burial gang (likely composed of convicts, the only Cruces residents who could be forced to serve as undertakers) waits outside, banging on the door, begging to be allowed entry, and servants, in the meantime, surround the corpse, struggling to dress her as befits her social station. Hierarchical social relations among the Panamanians persevere in death, a chilling normality where little in the way of normality is on offer.
Shortly after this episode, Seacole herself falls ill; in the nineteenth century as now, caretaker susceptibility to communicable disease was a major occupational hazard during epidemic outbreaks. Seacole’s struggle to recover, leaving the town briefly without the benefit of their chief cholera nurse. But her illness likewise provides a rallying point for Panamanian as well as foreign residents of Cruces, who come to her bedside hourly to monitor her progress: “Indeed, when I most wanted quiet, it was difficult to keep out the sympathizing Americans and sorrowing natives who came to inquire after me” (38). Seacole’s illness draws the different sectors of Cruces society together in the common hope of seeing their cholera nurse well again. It would be an exaggeration to suggest that the residents of Cruces overcame their differences in recognizing their shared dependence on Seacole, since the realities of life in the transit zone tended towards the creation of two unequal social spheres between the native-born population and the travelers from Europe and North America. Still, insofar as Seacole had treated them all without making distinctions between ethnicity, national origin, or ability to pay for her services, her illness made manifest the greater reality they shared: Everyone in Cruces lived in bodies that could get sick and die in a time and place where epidemic disease has struck. This recognition becomes a basis for a brief but powerful sense of collective experience.
Serious works of literature resonate in different ways across historical moments and circumstances. As our own twenty-first century pandemic forces us to collectively acknowledge the reality that we, too, inhabit bodies that can get sick and die, Seacole’s memoir offers lessons for the way we might begin to understand our own experiences. First, the Cholera’s—and Mary Seacole’s—presence in Panama points to the fact that pandemic disease neither emerges nor spreads without human intervention. It was British colonialism, and particularly British troops in India that helped the cholera bacterium travel beyond the regions where it first appeared. It was the development of an interconnected nineteenth-century world that enabled the disease to circle the globe. Panama’s status as a hub of transit and trade meant that the pandemic was guaranteed to eventually reach its shores, and the constant movement of new populations across the isthmus meant that new infections would continue to occur. The railroad brought Jamaicans to Panama, and a ship from Panama brought cholera to Jamaica; Seacole, like many other Jamaicans, moved to Panama in search of economic opportunity: As Jamaica fell into economic stagnation at midcentury, people emigrated to seek work on the Panama railroad or in the service and hospitality industry that had sprung up around the business of interoceanic transit. Seacole thought to escape the disease that had decimated Kingston, but because Panama played host to crowds of travelers from across the Americas, contagious disease transmission never really abated. Seacole found in Cruces a fresh outbreak of the cholera she had thought to leave behind in Kingston. In other words, it is not enough to say that capitalism and colonialism enabled epidemic disease; it is far more accurate to point out that, as the Chuang Collective has argued in “Social Contagion,” a widely-circulated essay from the early days of our own pandemic, human economic activity directly produces pandemics: In the case of COVID-19, this means heightened evolutionary pressures on viruses, which make them deadlier and more contagious, and industrialization of the countryside, which pushes humans into closer contact with wild animal species. As Chuang observes, “previously unknown viruses are essentially harvested from wild populations and distributed along global capital circuits.” In the case of cholera, too, global capital circuits provided a certain path for the spread of the disease. The gold rush brought travelers to Panama; the chance to make money off these travelers brought the steamship companies, the railroad company, and the economic migrants like Seacole and her brother; the perceived need to maintain order brought the military, and members of all these groups introduced, spread, and died from cholera. Early this year we might have been forgiven for believing that we’d left plagues behind, that here in the global North, at least, medical knowledge and public health policy had eradicated the possibility of falling victim to contagion. People in the nineteenth century could not have had such illusions. Seacole’s account of living through the disease reflects a range of responses we might now recognize as our own: shock, horror, and panic at the disease’s appearance combined with an appeal to social institutions like the church or the town doctor for relief. When these institutions fail, the people are left with the realization that they are on their own; it is then that the residents of Cruces turned to Seacole as the legitimate source of medical expertise. Seacole set to work tirelessly but carefully, doing what she could to save many and comfort the rest. Yet, it was not principally because of Seacole’s work that the cholera subsided: Medicine could treat patients, but not stop the epidemic. The outbreak ended only when it had burned its way through a substantial portion of the population of the town. Our final lesson from Seacole, then, might be that, like nineteenth-century residents of places where cholera struck, we find our fates tied to forces much greater than our powers to overcome them, and we trust our lives to those most prepared to act when disaster strikes. Yet the cholera epidemic, though it marked Mary Seacole’s life, represents neither her most formative experience, nor, ultimately, the most significant part of her legacy. In fact, Seacole’s descriptions of cholera comprise a surprisingly small section of her memoir. The Jamaica outbreak, which immediately preceded her emigration, is nearly written out of the story altogether, while the outbreak in Cruces is narrated in only a handful of pages. When the infections abate, the town begins the work of getting back to normal life. The travelers return, and Seacole opens her restaurant and inn, which she continues to operate in Cruces for many months. Proper mourning is nearly impossible: How can one effectively mourn so many deaths in so short a span? If Seacole’s narration preserves the affective charge of the epidemic, she likewise refuses to linger over or revisit the episode. The narration propels the text onward to new “wonderful adventures.” Does Seacole stage a kind of forgetting? Does she simply move on? Seacole’s story suggests, perhaps terrifyingly, that for the survivors whatever fears, privations, and suffering the epidemics brought soon came to be seen as a temporary ordeal, and, if not altogether erased, then soon enough pushed back into the recesses of memory. We have not yet lived to see if it will be the same with us.
Dennis M. Hogan is a PhD candidate in Comparative Literature at Brown University. He is writing a dissertation about the literature and culture of the transit zones of nineteenth-century Central America.
This post may contain affiliate links.
{kind=link}