In Coming Home, Wendy Kline has written a rich, illuminating, and engrossing history of the modern midwifery and home birth movement in the United States. As she writes, “While the book’s focus is on a specific type of birthplace and birth practitioner, it paints a broader picture of reproductive revolution and reform in modern America.” As one would expect, such a tale of reform and revolution in 20th century America involves a number of unexpected turns — for example, a vital link emerging between wealthy consumer rights activists in the D.C. suburbs and a caravan of 80 buses full of Bay Area psychedelic culture advocates in the 1970s. By unfolding these unlikely convergences and paradoxes over the course of nearly a century, Kline reconstructs the story of a set of under-appreciated radicals who, against long odds, fundamentally reshaped the conversation around birth and will continue to do so for years to come.

Wendy Kline is the Dema G. Seelye Chair in the History of Medicine at Purdue University. However, when we spoke she was in the United Kingdom with a family scattered by Covid-19 disrupted travel plans. The pandemic will lead to some overdue and fundamental conversations about health, healthcare systems, medical epistemology, and the important work of radical activists like those documented in Coming Home. The following conversation, in which we discussed the fractious politics of the 1970s, how midwives have a lot to each us about holistic medicine, and the status of the movement today, has been lightly edited for clarity.
Michael Schapira: Your prior book [Bodies of Knowledge] ended with a chapter on midwives. Was this always going to be the next project, or was it a discovery in the context of your past work that led to Coming Home?
Wendy Kline: It was absolutely discovery. That second book ended with a chapter almost exclusively about Fran Ventre and what happened in the Montgomery Country, D.C. area. It was really after I published it that I made personal communication with Fran. I was getting permission to use a photograph, but I had already finished the book. She and I started talking, and I think it was a combination of conversing with her and realizing how much bigger that story was that led to this book. It was also the fact that I had sort of gotten my foot in the door by writing the last book.
As you probably aren’t surprised to hear, a lot of midwives are very hesitant to open up about their stories, because they’ve been persecuted for doing so. So I started hearing more stories. First with Fran, who told me a lot of stuff that wasn’t in the archive, and then she started connecting me with other people.
I met Ina May Gaskin on the Farm just after Bodies of Knowledge came out. I went for a workshop and I gave her a copy. She happened to be just finishing up one of her books and integrated a little of my material into her book. That combination of factors suddenly opened up this whole world of additional stories and material, and I thought, “Oh my gosh, how could I not keep writing about this?”
I knew very little about the movement before I came across Fran’s material at Harvard. But there was such a huge story there, it’s so rich.
You mention Judith Walzer Leavitt’s Brought to Bed as a pathbreaking book, but what was the state of historical scholarship on this topic when you began working on Coming Home?
I struggled as I began the writing. I asked myself, “is this really a story about midwives, or is this a story about homebirth?” The book turned out to be a combination of the two, but in terms of the scholarship most of the stuff that had been written was more about Certified Nurse Midwives, or a longer trajectory about childbirth. There was not a whole lot about what happened in the 70s. I think that’s partly because of the lack of materials. So much of the research I did for this book, I got out of people’s attics and garages. So many of them hadn’t come to terms with the fact that what they had done was historically significant; that they should preserve some of this material and put it in an archive. One of the reasons why less had been written about people like them and that particular time and history of the movement was just that people didn’t know how to access the stories. They were more or less invisible.
As a historian, it’s interesting to me. That was 50 years ago, but it still seems for many people that it’s not quite history; it’s too recent. From a historical perspective there is just so much more that has been written about earlier time periods, not just in terms of childbirth, but in general.
I started feeling that people had a hard time taking the 1970s seriously. This story is wrapped up in a larger story about the counterculture, and it’s taken people a while to really look into things that took place in the counterculture either as relevant or historically significant. Instead we see this as a blip on the screen.
I wanted to ask about the 70s specifically. There are two trajectories that eventually will coalesce into the midwife movement – the Consumer Rights Movement and the Counterculture. I think both are becoming more relevant today as people rethink the limits of different political strategies. Because you brought up Fran Ventre already, I was wondering whether going into this Consumer Rights aspect of the history has led you think about the enduring possibilities and limitations of this approach.
It’s not hugely easy for me to answer. This story is hard to place on the political spectrum. My expertise is in the area of feminism and feminist health, but you have participants in the midwife movement that do not at all identify with feminism or feminist health. Some of these consumer groups that get really involved argue from the perspective of being a consumer having a right to make their own decisions, and represent themselves, and a lot of them were pretty far to the right. This led to a bit of an uneasy alliance between some of the players. Some of the consumer activists didn’t really agree with what some of the more feminist midwives were pushing for.
However, I think they realized that the combination could be quite powerful. You had a profession that was really trying to establish itself and gain some scientific or medical legitimacy, and then it’s backed by a bunch of non-scientists, non-medical professionals who were saying “we demand this,” so that it brings in that economic and market component. They said, “we’re going to go for this whether you like it or not, so if you don’t provide it, we’re gonna go elsewhere.” I think the two actually do fit together. They thought, if we can bring our agenda together, then we can actually succeed.
The other thing that is going on is that in the 1970s, within the history of medicine and the medical marketplace, the consumer is getting a louder voice. There is a recognition that they can serve on committees, they can do research on their own, and they are gaining greater visibility and credibility. If you want to initiate change at any point you better listen to them, and you better get on their good side.
I don’t remember how much I included this in the book, but you had conferences between consumer groups and midwives – one was at the Farm. It was a NAPSAC meeting – The National Association of Parents & Professionals for Safe Alternatives in Childbirth. That was a weird group of consumers and midwives and some doctors. I’d love to be a fly on the wall for a meeting like that. The stakeholders all have different interests involved.
There are so many of these contradictory energies in the movement. There is this push for consumer advocacy, there is a push for professionalizing midwifery, and then there is a push for redefining the status of childbirth to take it out of the medical context. It’s very fascinating to see this play out for the nearly 100 years that you cover in the book. Is the movement, from your observation and having talked to a lot of people for the book, still fragmented in how people understand what they are advocating for and doing, or have you noticed more consensus?
It’s a bit of an up and down. There is a lot of division between the organization that represents Certified Nurse Midwives, the ACNM, and MANA, which basically represents the Certified Professional Midwives. There are a couple points of contention between them, but the biggest is over the question of midwifery education and forms of apprenticeship learning. Can you get licensed and accredited without going through the traditional classroom route? That’s been a source of huge divide between the two groups.
There are bigger issues of course, like the location of birth – home, hospital, or birth center. Race has been a big issue, as well as homophobia – so the kinds of things that you see in other professional organizations are a major issue with them as well. There is still quite a bit of tension between the two groups, but they have made some progress. For three years in a row there was a meeting called The Summit, which I attended. It was an attempt to have a conversation with all the stakeholders and come to some sort of resolution.
The Summit is an interesting example. In the book there is a section on something called “Dialogue Day” that has a similar aim. Narrative is a through line in this movement – especially in making narratives around birth available when they’ve been suppressed by making birth a medical event. It reminded me a lot of developments in medical education today, for example the Narrative Medicine program at Columbia. In this sense midwives were way ahead of developments in medical education. In doing the research did you gain a sense of how revolutionary this movement was, now that some of their critiques have been accepted as commonplace 40 to 50 years later?
I see what you’re saying. I came to this project after writing Bodies of Knowledge. One of my big arguments there was that what the feminist health movement really did was change the way that we understand evidence and experience – and actually the knowledge of the body. Individual experience can be as legitimate as scientific knowledge. There is a form of embodied knowledge that up until the early 70s had been left out of the equation. That required listening to individual stories, so stories become almost a part of the testimony that helped to shift the dialogue, shift our understanding of what medicine is doing, what health is about, all of those things.
That was already in my head when I was writing this book. I felt like this was one example of that larger shift that was taking place. Midwives were recognizing and redefining what the experience of childbirth was. And the only really effective way, or one really effective way of doing that, was to tell the stories. Without the stories childbirth just becomes an anatomical, physiological, medical event.
My favorite example of that is something I include whenever I do a presentation on the Bowland Bust, the Kate Bowland story. I’ll show an image from her journal, which is a record of a birth – she’s timing contractions – but she’s also drawing pictures of the laboring mother and she’s got notes on The Communist Manifesto. To me that illustrated this very different holistic approach. Birth was all of those things, all at once. Timing a contraction also involved reflection and artistry and stories and everything else. Getting my hands on her diary blew my mind, being able to see all of those things in process. This speaks to what I’d call holistic medicine. You have to look at something from all these different components in order to really understand what it’s about.
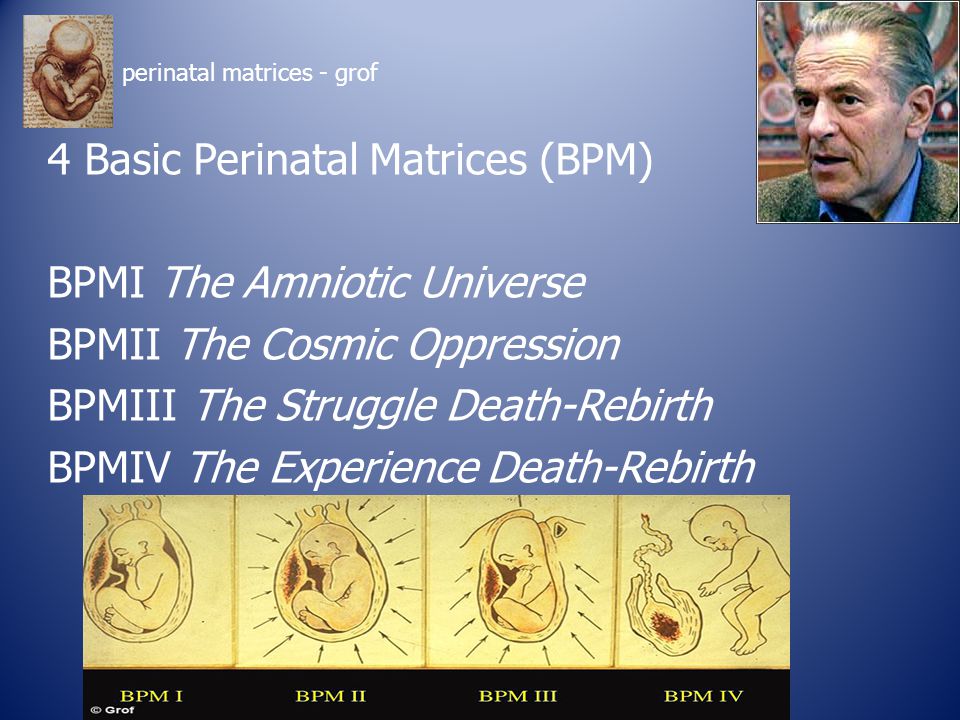
I think the most provocative chapter is about The Farm and the relationship between research in psychedelics and literature that grows up around the midwife movement like Spiritual Midwifery. In the 1970s it’s a strange moment where you have doctors and researchers thinking in this holistic sense. For example, there are things in the book like Stanislav Grof’s chart on Basic Perinatal Matrices. [Grof was an early researcher of LSD.] You get a sense that scientific research was more pluralistic back then.
That’s a good point. I have to tell you about Grof. He first showed up in Kate Bowland’s diaries. She kept referring to someone named Grof, and she would put BPM 1, BPM 2, which referred to his Basic Perinatal Matrices. But I didn’t know what this was at the time. Then I interviewed Raven Lang, who was very science oriented and was always reading all kinds of materials. She said Stan Grof was very important, but I had no idea who he was. So I sit down and Google his name and it lo and behold his papers are at Purdue University, where I teach! I said, “you’ve gotta be kidding me.” So it became very easy to do that part of the research because it was right there under my nose the whole time. The project I’m working on now is on LSD, moving beyond the whole childbirth story, and I’ve got all of this amazing archival material to use.
You’re in the UK at the moment, and I had a question about popular representations of homebirth and midwifery. The book opens with Gisele Bündchen celebrating her homebirth and noting how it has become popular amongst celebrities, and in UK Call the Midwife has been such a popular show. In sharing this work in different contexts, do you find that people have different expectations that are mediated by popular representations of homebirth and midwifery?
They do, but for the majority these expectations are incredibly limited. Most audiences, especially in the US, know nothing except what they might have been exposed to in popular culture when it comes to childbirth. They assume that all of this disappeared long ago. They are surprised that midwives still exist, they have no idea that there are various types of midwives, which I think is a really important part of the story, and one of the reasons why it’s so complicated and very different from places like the UK. If anything, they won’t associate with the British Call the Midwife model at all, unless they’ve seen the show. They’ll associate it more with Ina May Gaskin, counter-cultural hippies. It’s a hippie thing that’s been fully invalidated as being socially irresponsible; all of that baggage about how dangerous childbirth is. Especially amongst younger audiences, whatever they are exposed to birth in popular culture, it’s all about the danger of birth. You rush to the hospital and nearly die if it weren’t for an emergency C-section. They’ve been indoctrinated into that hyper-medical model and are just surprised that I would even be bothering to talk about this wacky group of people.
And in the UK I take it that things are quite different, because the associations would be different.
Yeah, but it’s also that the history is so different because they weren’t eliminated. Midwives were absolutely integrated into the medical system here [in the UK]. It’s still a very medicalized model – most babies are born in hospitals. It may be under the direction of a midwife, but they are making very similar decisions to what an OBGYN would be making in a hospital setting.
If I’m giving a talk and the audience doesn’t really know anything about the status of midwifery in the US I start with a couple of statistics. I might get these numbers slightly wrong, but you’ll get the general idea. In the US there are something like 15,000 midwives and 30,000 OBYGNs. In the UK there are about 30,000 midwives and 1,600 OBGYNs. If all you know are these ratios, it’s clear that you’ve got one culture in which midwives are pretty much running the show and OBGYNs are reserved for true medical emergencies, and in the US you have OBGYNs absolutely dominating the field. So there’s that point about professionalization.
My next point is the fact that the US is one of the most expensive places in the world to give birth and one of the least safe. What does that mean? We’re spending all of this money, we’ve got all of these OBGYNs, so why is birth less safe?
Midwives were virtually eliminated in the US and in most countries they were part of the larger model, so they work in tandem with hospitals and doctors. That is why Americans are largely ignorant about the whole storyline.
It will be interesting to see how this pandemic changes some of these attitudes.
Reading the book in the context of the pandemic raised a lot of questions. Health care was also front and center in the Democratic primaries and has become one of the defining topics of our politics. It seems like there is a lot to be learned from the midwifery movement. Is there anything that stands out to you in light of current events?
It does make me wish that more people in power would read books like mine or any books that remind us of the broader history of health and medicine in the US. I get frustrated by the current debates that go on, even in professional midwifery organizations. You get the sense that they haven’t learned and are repeating the same arguments that were made 40 years ago. Part of this is just a power mechanism. Even Certified Nurse Midwives in hospitals have very limited power in shaping how our medical system works. If you add licensure and health insurance and all those sorts of things you can see how they are still relatively powerless.
The work that these midwives and consumer advocate groups did in the 70s was phenomenal. They poured their heart and soul and energy and time for very little remuneration, but with a passion to fix what they saw as being fundamentally wrong with the healthcare system. Yet here we are having the same debates.
One thing has changed really recently. In 2014 Britain changed its recommendation for pregnant women who were low risk. It was based on this large study – the British Birthplace Study – that tracked births in four locations: in hospitals, at home, in birth centers that were physically attached to hospitals, and then stand-alone birth centers. It involved 64,000 births and they basically found that proximity to the operating room completely transformed your likelihood of having a C-section. If you took away all of the risks, it was simply if you were in a hospital, you were four to eight times more likely to end up having a C-section. For that reason, the National Institute for Health and Care Excellence issued new guidelines, suggesting that midwife-led units were safer than hospital for low-risk women.
That comes in 2014. Everybody in the US balks at this. The New York Times does a whole series challenging this and there is a flurry of responses. Harvard obstetrician Neel Shah wrote a piece for the New England Journal of Medicine which basically said, you know what, “obstetricians like me may be hardwired to operate, and too many operations are harmful to patients.” Maybe patients should stay away from obstetricians, unless they really need one. But people in 2014 for the most part thought the UK recommendations were ridiculous, or at least unworkable in the US, that there was no way it could be safer to stay out the hospital than to go in. This [i.e. the Covid-19 pandemic] is going to change that debate. If I were pregnant right now, even if I knew nothing about midwifery and homebirth, I would start questioning whether I wanted to set foot in a hospital, period. I know that midwives are getting calls right and left in places like New York City, where people understandably are recognizing that maybe they don’t want to give birth in a hospital.
The larger issue comes back to childbirth and whether it is a medical procedure, or if it’s something physiological. If you’re well-prepared and educated and you have a backup plan, the experience could be far safer and more meaningful if you just stayed away from the hospital. It’s too early to tell, but the pandemic could really shift the debate.
Also, this is not just about consumer interest, but in integrating midwives into the larger healthcare system – recognizing that this could be cost-effective as well as safe, a better use of resources, and lead to better birth outcomes. It’s not just about the individual pregnant woman with her partner who decides that during this particular pandemic they would like to stay out of the hospital, but a larger question about what the role of hospital in all of this should be.
Have you ever done research that has involved doing so many interviews, instead of relying primarily on archival material?
My first book was on eugenics, no interviews. The second one had a few, but not nearly as many as this one.
The reason I ask is related to a question that I had trouble forming. In Coming Home I kept seeing the parallels between debates within the historical profession about standards of objectivity and those within midwifery about standards of medical competence. Those debates about professional standards were evolving over the course of the 20th century in medicine, but also in history. In doing work that involves interviews with living people and more recent history, which may not have been accepted at certain points by professional historians, I was wondering if this project led you to revisit some of these debates about what it means to set baseline professional standards.
From a practical viewpoint I sort of go in two directions. As a medical historian, but as a women’s historian first, I’ve developed an appreciation for creativity of sources. If you want to write something other than the standard history, you have to look differently. You have to explore in more creative ways to find sources. I’m thinking of Laurel Thatcher Ulrich’s A Midwife’s Tale. That means seeking out people – oral histories – but also being creative about what actual sources might exist. And a lot of times it’s in somebody’s attic or basement. Challenging the historical profession to think more creatively about how we might find evidence and what we do with that evidence is one viewpoint.
On the other hand, I have become, especially in this past year based on some reading I’ve done, distrustful of memory. Every person that I interview, they are trying to recall something from a while back, and they have their own agenda about how they want to be remembered. In an ideal situation I have two things. I have some evidence – letters they wrote or a journal, that I can then supplement with an interview to help flesh out what I think the story was. But problems can ensue if you rely too heavily on one or the other. Anyone who does recent history should take advantage of the fact that you have living people out there who can flesh out your story, but you also have to think twice about how reliable memory is to you in this story.
And what about this question of professionalization?
I see the other sense of your question. I remember reading That Noble Dream, but it was in my first year of grad school, which was a long time ago. I can see that this is a story of professionalization, and models, and how, I don’t know if threatening is the right word, but how confusing it can be when who had previously been deemed outsiders with a different base of knowledge come to be seen as threatening to another group’s power, authority, or legitimacy. This results in a more general conversation about who we are and what our primary goal is, whether as historians or as childbirth educators or practitioners. What is it that we do, and how do we do it well? That can be a really disarming question if a different group is being included in the conversation.
So there is the profession on one side, but there is also the question of education. I wasn’t intending to do a whole bunch of research on midwifery education, but then I realized I had to in order to write this book. It made me think more generally. If you re-invented something, if you had a group of people come together and say, “This is what we think childbirth should look like. This is the setting and the model, and you guys have it wrong, and we’re going to propose something different.” Well, in order to get legitimacy in the eyes of the state you need to get accredited, which means you have to start a school, which means you have to ask, what does the school look like? What does the curriculum look like? That is a really interesting exercise, because it is less about childbirth per se, and more about the decisions that have to be made about creating and sustaining a model. Looking through the records of the Seattle Midwifery School I found myself exhausted – all of the stuff they had to educate themselves on, just to create a model that they then had to use to train themselves, and then to continue with it to draw in students. It’s amazing that they were able to do that, because it really was against all odds.
And it’s such an interesting juxtaposition with the El Paso meeting. There are these two moments that attempt to define the status of midwifery, or the politics of homebirth. In El Paso there are all of these debates about how much to trust people form the medical profession, and what values the midwife movement should endorse. That is a question about definition and political priorities. But the next chapter is about starting a school, which is a completely different exercise in defining your purpose.
It was very hard to write because there is a huge overlap in who the educators are and who the reformers are. They are all in the same group, and yet there are these moments when they find themselves pulled apart. That also has something to do with radicalism and to what extent you buy into the system. If what is holding you back is that you are outside of the system, then you might want to create an educational program to become legal, to become recognized. But each time you make those decisions someone is going to say that you’ve sold out to the medical model. That is one of the sadder aspects of this movement, the extent to which those decisions ended up pulling people apart rather than bringing them together.
Things look different today. The midwifery profession has come a long way in the U.S. Diversity and inclusion are taken far more seriously. Technology and even social media have enabled organizations to portray themselves – and the state of the profession – more coherently. There are more midwifery programs, greater opportunities, more attempts to impact research and engage in a larger conversation about birth outcomes. The danger, I believe, is that it’s too easy to lose sight of the history of the profession and the struggles that earlier generations of women faced as they struggled to organize, educate, and gain legitimacy. We need to remember their stories and their struggles, their faults and their strengths, as we continue to navigate an increasingly complex health care system.
Michael Schapira is an Interviews Editor for Full Stop.
This post may contain affiliate links.
{kind=link}